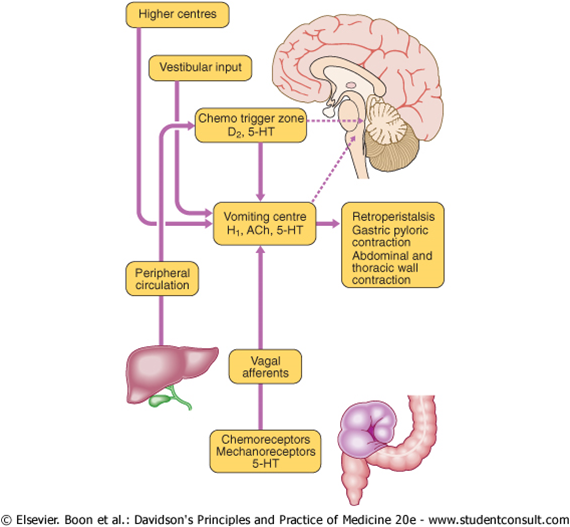
Vomiting is controlled by the area postrema lying inferior and posterior to the 4th ventricle in the medulla. There is the chemoreceptor trigger zone (CTZ) and the vomiting centre. The vomiting centre receives afferents from GI (eg mucosal irritation), extra GI (eg bile duct and other organs), extra medullary (eg vestibular and olfactory systems) and CTZ. CTZ detects blood born toxins.
Antiemetic antihistamines (H1): eg cyclizine, cinnarizine. Used in motion sickness and vestibular disorders. Acts on vomition centre.
Dopamine 2 antagonists: eg domperidone and metoclopramide. Act on CTZ. Note: domperidone does not cross BBB therefore no dyskinetic side effects.
Serotonin receptor antagonists: eg ondansetron. Used in nausea and vomiting especially associated with cytotoxic medication as they act on CTZ.
Anticholinergics: eg hyoscine. Effective in motion sickness and gastric irritation. Do not act on CTZ.
Phenothiazines: eg chlorpromazine. Act mainly on D2 receptors. Can also block histamine and muscarinic receptors. Commonly used in severe N&V associated with vertigo.





